

The first man died in April 2014. Another died later that month. Then on July 18 of that year, a woman was rushed to a hospital where she was told she was lucky to be alive.
They all went to the same Little Rock, Ark., surgery center for a colonoscopy, among the safest procedures a patient can have. And each stopped breathing soon afterward, court records say, sustaining the same type of brain damage seen in a drowning victim.
What happened at Kanis Endoscopy Center prompted no review by officials in Arkansas, which, like 16 other states, has no mandate to report patient deaths after surgery center care. So no facility oversight authority has examined whether the deaths were a statistical anomaly or cause for alarm.
A Kaiser Health News and USA Today Network investigation found that surgery centers operate under such an uneven mix of rules across U.S. states that fatalities or serious injuries can result in no warning to government officials, much less to potential patients. The gaps in oversight enable centers hit with federal regulators’ toughest sanctions to keep operating, according to interviews, a review of hundreds of pages of court filings and government records obtained under open records laws. No rule stops a doctor exiled by a hospital for misconduct from opening a surgery center down the street.
Even the high-profile death of comedian Joan Rivers — who passed away in 2014 following a routine procedure at a Manhattan surgery center — failed to appear in Medicare’s public tally of patients rushed to a hospital.
When Faye Watkins, 63, walked into Kanis Endoscopy in Arkansas, she was unaware that there had been two deaths after care there within the previous three months, she said. She was in the fog of anesthesia when it struck her that something was amiss. She said she heard men say her blood pressure was falling.
“I said [to myself], ‘Lord, if it’s time for me to go, take me. But I’m not ready,’” Watkins recalled. Her next memory was waking up in a hospital with her chest sore from CPR.

The KHN/USA Today examination raises questions about the need for more robust oversight of surgery centers, where public access to important information, such as surgical outcome data, tends to be more limited than what’s available about hospitals. The gap persists even as the nation’s 5,600 surgery centers have surpassed hospitals in number and taken on increasingly complex procedures.
“It’s disgraceful that there’s so little information” about what happens in surgery centers, said Leah Binder, chief executive of the Leapfrog Group, an employer consortium that surveys more than 2,000 hospitals a year.
Scrutinizing unexpected deaths is the norm for U.S. hospitals. The Joint Commission, their leading accreditation body, recommends that members send the accreditor reports of unexpected deaths so that lessons from one tragedy might prevent another. The top surgery center accreditation body has no similar guideline.
Bill Prentice, executive director of the Ambulatory Surgery Center Association, an organization that represents the centers in policymaking discussions, said the centers safely perform millions of procedures, from tonsillectomies to knee replacements, each year.
Prentice said he supports giving patients access to data that could compare surgery centers with hospital outpatient departments.
“We shouldn’t have a patchwork system where one state asks for one thing and others ask for others,” Prentice said. “What consumers want is consistency.”
Colorado requires surgery centers to report deaths and some major injuries to the state health department, and the agency posts summaries of incidents online for consumers. Several other states — including Pennsylvania, Florida and New Jersey — require incident reports but don’t reveal to the public where they happened.
In at least 17 states, health facility officials confirmed they have no way to know that a patient died because surgery centers have no duty to report. So just as in Arkansas, surgery centers had no mandate to notify an official over cases outlined in lawsuits, including a 33-year-old Missouri man who died after finger surgery, a 66-year-old Georgia woman who died after an eye procedure or a 60-year-old in Oklahoma who died soon after a total hip replacement.

Robbin Smith’s legal team argued that the center should have ensured that its doctors did not use the drug Kenalog — an injectable steroid — for epidural injections. The drugmaker had changed the label in 2011 to warn against using it that way due to the risk of paralysis. (Austin Humphreys/The Coloradoan)
Even in Colorado, a leader in transparency, the outcome of a 2017 jury trial raised questions about the depth of the oversight. Robbin Smith was paralyzed from the waist down after an epidural pain injection at the Surgery Center at Lone Tree in 2013, according to her lawsuit against the center.
Smith’s attorneys cited Medicare rules that say the center’s own governing body has a duty to keep patients safe. Each center must appoint a body that is legally responsible for the center’s operations.
Smith’s legal team argued that the center should have upheld its duty by ensuring that its doctors did not use the drug Kenalog — an injectable steroid — for epidural injections. The drugmaker had changed the label in 2011 to warn against using it that way due to the risk of paralysis.


Jurors ultimately ruled against the Surgery Center at Lone Tree, awarding Robbin Smith $14.9 million. The center has filed a motion for a new trial. (Courtesy of Robbin Smith)
The center’s governing body never discussed proper usage of the drug prior to Smith’s care, trial testimony shows, and there’s no sign that state or private facility overseers examined the board’s actions before Smith’s injury.
The surgery center’s lawyer argued that the doctor — not the facility — was responsible for choosing Kenalog for Smith’s treatment. The doctor denied wrongdoing and reached a confidential settlement with Smith before her case against the center went to trial.
Jurors ultimately ruled against the center, awarding Smith $14.9 million. The center has filed a motion for a new trial.
Public Reports Flawed
The federal government posts on its “Hospital Compare” website far more data about hospitals than surgery centers, and available hospital data cover several types of surgical complications and mortality rates for certain conditions. Some hospitals’ quality measures, like infection rates or patient satisfaction scores, reflect the experience of every patient in the hospital.
The same Medicare website displays different data for surgery centers — and for some key measures, the reported results cover only a fraction of patients. Medicare allows surgery centers to report data for as few as half of just their Medicare patients, ignoring most patients under age 65 who do not yet qualify for Medicare.
In practice, that has allowed surgery centers to report as many hospital transfers as they choose — unless more than half of their patients leave by ambulance.
Yet a person examining the data on the Medicare website would see no explanation about the limits of the information. They would see a national transfer rate that’s less than half the rate reported in medical research.
State records, ambulance records and Medicare’s own inspection reports highlight the apparent disconnect. They show that dozens of centers reporting zero transfers in Medicare’s public data do, in fact, send patients to hospitals.
For example, Memphis-based Urocenter, which specializes in urological procedures, reported to state officials 45 transfers combined in 2014 and 2015. Its public report on the Medicare website for those years showed zero transfers.
When a reporter noted the discrepancy, Urocenter’s administrator responded in an email that the facility “put in place corrective measures … and have provided [Medicare] with the corrected information.”
The Medicare data also show zero transfers in 2014 from Yorkville Endoscopy. The Manhattan surgery center transferred Joan Rivers, 81, to a hospital after complications from a vocal cords procedure that year. Rivers died a week later.

An attorney for Yorkville Endoscopy said all transfers meeting the government’s standards were reported.
After reviewing the reporting rules, Cheryl Damberg, a Rand Corp. researcher who has worked on hospital quality-reporting tools for the federal government, said the 50 percent rule leaves the public with little useful information.
“It seems like this can totally be gamed,” Damberg said. “From a consumer standing, the data [for surgery centers] doesn’t have a lot of utility at this point.”


Bill Prentice, executive director of the Ambulatory Surgery Center Association, said he supports giving patients access to data that could compare surgery centers with hospital outpatient departments. (Courtesy of Ambulatory Surgery Center Association)
Medicare officials said in an interview that the agency allows limited reporting so the requirements do not overburden surgery centers.
Yet industry leaders have told Medicare they want to report more data. In letters to Medicare during 2016 and 2017 rule-making periods, the ASC Quality Collaboration, a group of surgery center leaders, urged Medicare to collect reports on every patient transfer to expand transparency and accountability.
Medicare made a very different move in July, proposing to stop collecting surgery center-to-hospital transfer data and seven other measures of quality. The agency said it still plans to report on incidents gleaned from its own records, like visits to the hospital seven days after certain surgery center procedures.
Medicare said in the proposed rule that the transfer measure appears to be “topped out,” meaning there is a tiny difference in transfer rates reported by the centers.
Dr. Ashish Jha, a senior associate dean at Harvard’s School of Public Health, said calling the data “topped out” is puzzling since Medicare is not sampling all of the patients.
“Getting rid of [the transfer measure] doesn’t make a lot of sense to me,” he said.
Prentice, of the surgery center association, lauded the proposal in a press release as recognizing the “outstanding” work of surgery centers in preventing harm. In an interview, he conceded that he was “parroting” Medicare’s sentiment and said he hopes the industry will find a way to report meaningful quality data.
“I want us to fill that gap,” Prentice said. “We need to be robustly reporting data to [Medicare] and the world on quality of care.”

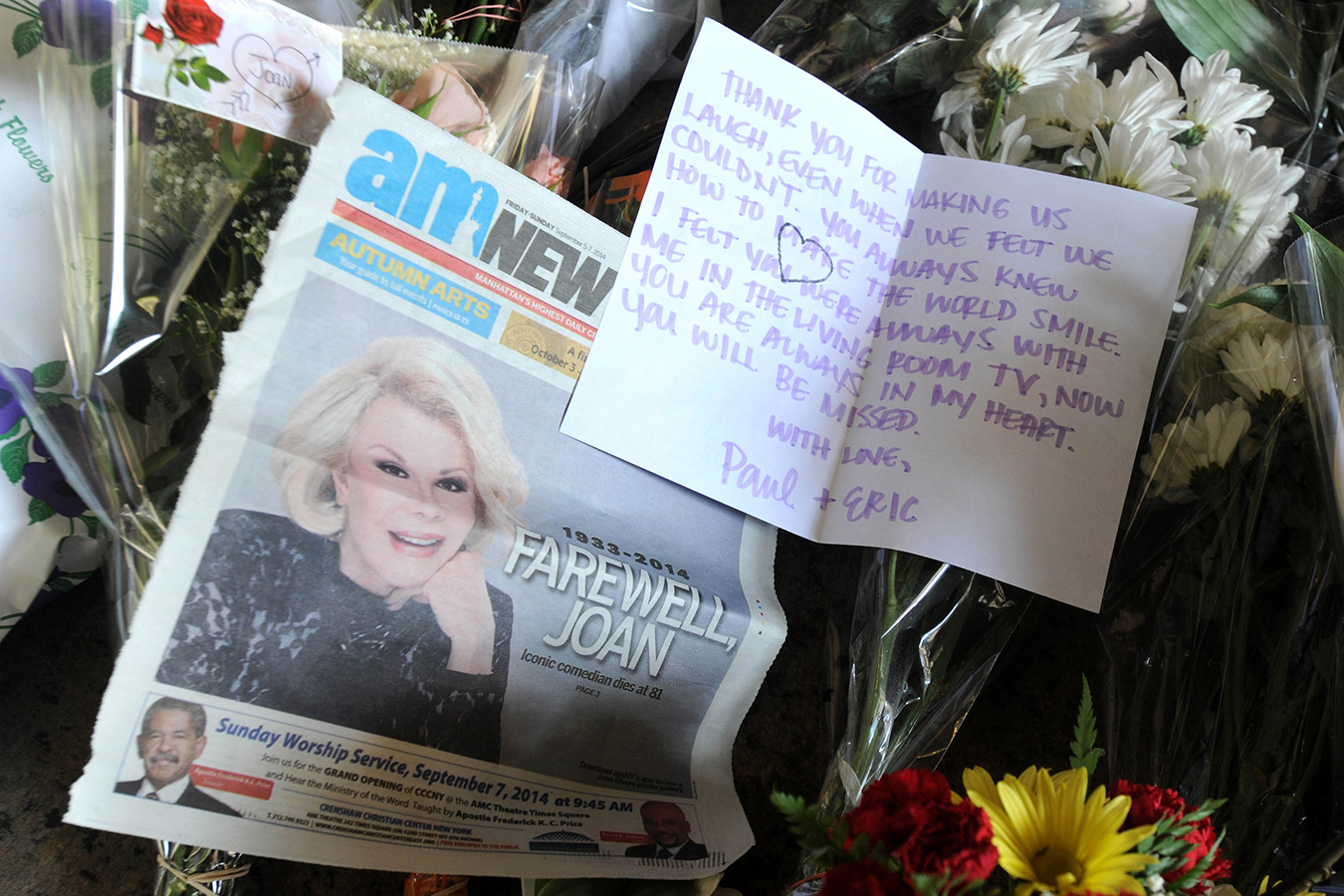
A memorial of cards and flowers lies outside Joan Rivers’ apartment in New York City in 2014 following the comedian’s death. Rivers passed away after a routine procedure at a Manhattan surgery center. (DVT/Star Max/GC Images)
Cluster Of Cases In Arkansas
Medicare’s rules for surgery centers require them to track unusual events, analyze them internally and try to learn from them. But after two deaths and a close call after procedures at Kanis Endoscopy Center, no outside official went in to see if patients remained at risk.
Medicare spokesman Tony Salters confirmed that, lacking a consumer complaint, no state or federal official was notified of the events and no special review occurred.


In April 2014, Rev. Ronald Smith died at a hospital after visiting Kanis Endoscopy Center for a colonoscopy. (Courtesy of Deborah Smith)
Yet what happened in a stretch of three months was far from routine. In April 2014, Rev. Ronald Smith, 63, died at a hospital after visiting Kanis for a colonoscopy. His family later alleged in a lawsuit that Smith’s sleep apnea and heart disease made him “extremely high risk” for undergoing anesthesia at the center, rather than at a hospital.
Smith was close to death at the Little Rock hospital when, coincidentally, an Arkansas health official began a routine inspection of the center on behalf of Medicare, records show. The lack of public information makes it impossible to determine precisely what happened in Smith’s case.
Medicare spokesman Bob Moos said state recertification inspectors come in every four to seven years and review all cases in the previous year in which a surgery center patient was transferred to a hospital. When the state inspector visited Kanis, “nothing on the hospital transfer log raised a red flag for her to investigate,” the spokesman said.
Officials would not describe what was on the transfer log or which cases were on it or confirm that Smith’s name had been included on it.
A Kanis spokesperson said it would violate patient confidentiality to comment on what the staff showed the inspector. Arkansas Department of Health spokeswoman Meg Mirivel provided no details, saying state law prohibits releasing information about hospital or surgery center investigations.
The state official’s inspection report does not mention any patient transfers. It does say the center was operating outside of industry norms by performing colonoscopies without an additional nurse in the room. The center pledged to health officials that it would add a nurse to the endoscopy suites.
The extra set of hands can be critical in case of an airway failure, said Dr. John Dombrowski, an anesthesiologist and a board officer with the American Society of Anesthesiologists.
“When you have an airway problem, you’ve got minutes,” he said. “When you have more hands on deck, you’re better able to save somebody.”
About three hours after the inspector left Kanis, another ambulance was speeding to the center.
It remains unclear if having another medical professional present would have helped save Clarence Creggett, 83, who also stopped breathing at the center after his colonoscopy, according to his family’s lawsuit. He died in a hospital nine days later, the family alleged.
Creggett’s family also filed a lawsuit, alleging that he was at “extremely high risk” as a surgery center patient, given his age and history of respiratory problems, including asthma.
Watkins, who survived after she stopped breathing, according to her lawsuit, said she only learned about the deaths of Smith and Creggett through gossip at her bank and hair salon. “My eyes got big then,” Watkins said. “That’s how I actually found out.”
Attorney Lamar Porter filed lawsuits in Pulaski County, Arkansas, on behalf of Watkins and the families of Smith and Creggett. The suit alleged that Dr. Alonzo Williams, who performed all three procedures, failed to properly screen the patients. The suits also claim that the nurse anesthetists did not administer the anesthesia appropriately.


“I said [to myself], ‘Lord, if it’s time for me to go, take me. But I’m not ready,’” Faye Watkins recalled thinking during her procedure at Kanis Endoscopy in Arkansas. (Robert Huston for KHN/USA Today)
The anesthetists also denied fault or negligence in legal filings. Dustin Wixson, the nurse anesthetist on the Creggett case, said the death was the only one in his 14-year career.
Williams denied wrongdoing in court filings for each case. He did not respond to requests for comment. Siegler’s letter stated that he was dismissed from the lawsuits before they settled and has “practiced for over 35 years with an unassailable reputation nationally. He was appointed by three separate Arkansas Governors to [the] Arkansas State Medical Board.”
Crackdowns That Don’t Stick
Medicare inspectors have a harsh sanction they mete out sparingly after serious safety lapses: involuntary decertification. It means the federal government won’t pay for seniors’ care at a health facility.
Such actions cut off a major source of patients and payments to hospitals and tend to make headlines. Hospitals that were involuntarily decertified in recent years closed for good, had to reopen as a clinic or reorganized before seeing another patient.
But surgery centers hit by such penalties have hardly skipped a beat.
Medicare pulled its certification from Cascade Cosmetic Surgery Center in Orem, Utah, on Dec. 28, 2014, after state inspectors said the center failed to meet basic standards mandated by federal regulations.
Medicare requires a surgery center to have a governing body that has formal meetings and takes legal responsibility for providing “quality health care in a safe environment.” According to the inspection report, the Utah center’s owner, Dr. Trenton Jones, told the inspector “he was the governing body and that he did not keep minutes of his thoughts.”
The inspection also said the center did not meet Medicare’s infection-control rules, such as putting a licensed professional in charge, determining what kind of bacteria infected patients or logging antibiotic use.
In some states, licensing officials would follow Medicare’s lead and revoke their approval. But in Utah, any licensed surgeon can operate in a one-operating-room surgery center without state approval, said Tom Hudachko, spokesman for the Utah Department of Health.
That meant Cascade was open for business — five days after Medicare pulled its approval — when Sandy Lee Walters, a 37-year-old real estate agent and mother of three, flew to Utah from Hawaii for breast reduction, tummy tuck and liposuction surgeries. The procedures took nearly nine hours, from 2:30 p.m. to 11:20 p.m., court records show.
Five days later, Walters died after a blood clot lodged in her lung. Her autopsy report notes “recent surgery” as a “significant contributing condition” in her death.
A lawsuit filed by her family alleged that Walters was at high risk for a blood clot because of her recent air travel and the extent of the surgery, yet she was not prescribed a “sequential” compression device or clot-busting medication. The suit is ongoing.
Walters’ eldest daughter testified in a deposition that her brother treasures a blanket his grandmother made from his mother’s blue jeans. “We all have a little piece of us missing,” the teen testified.
Three months after Walters’ death, a 55-year-old woman went to the same surgery center to have her breast implants removed. Within a week, the woman was found to have infections so severe that her nipples had to be removed in subsequent surgeries. In 2017, the woman filed a lawsuit alleging malpractice by Jones and the center. The suit is ongoing.
Cascade, Jones and his attorneys did not return calls or emails seeking comment. In both lawsuits, Cascade and Jones denied the allegations, according to court documents.
In California, eight centers that Medicare decertified over health violations have continued to operate on patients, with the blessing of private accreditation agencies hired by the centers to perform inspections. They include a center that was operating without a lifesaving drug in the crash cart and a facility where managers pressed an unqualified receptionist into duty disinfecting scopes used inside the body.
A Medicare official said accreditation bodies are notified when the agency pulls an approval, but officials do not control the private body’s decisions.
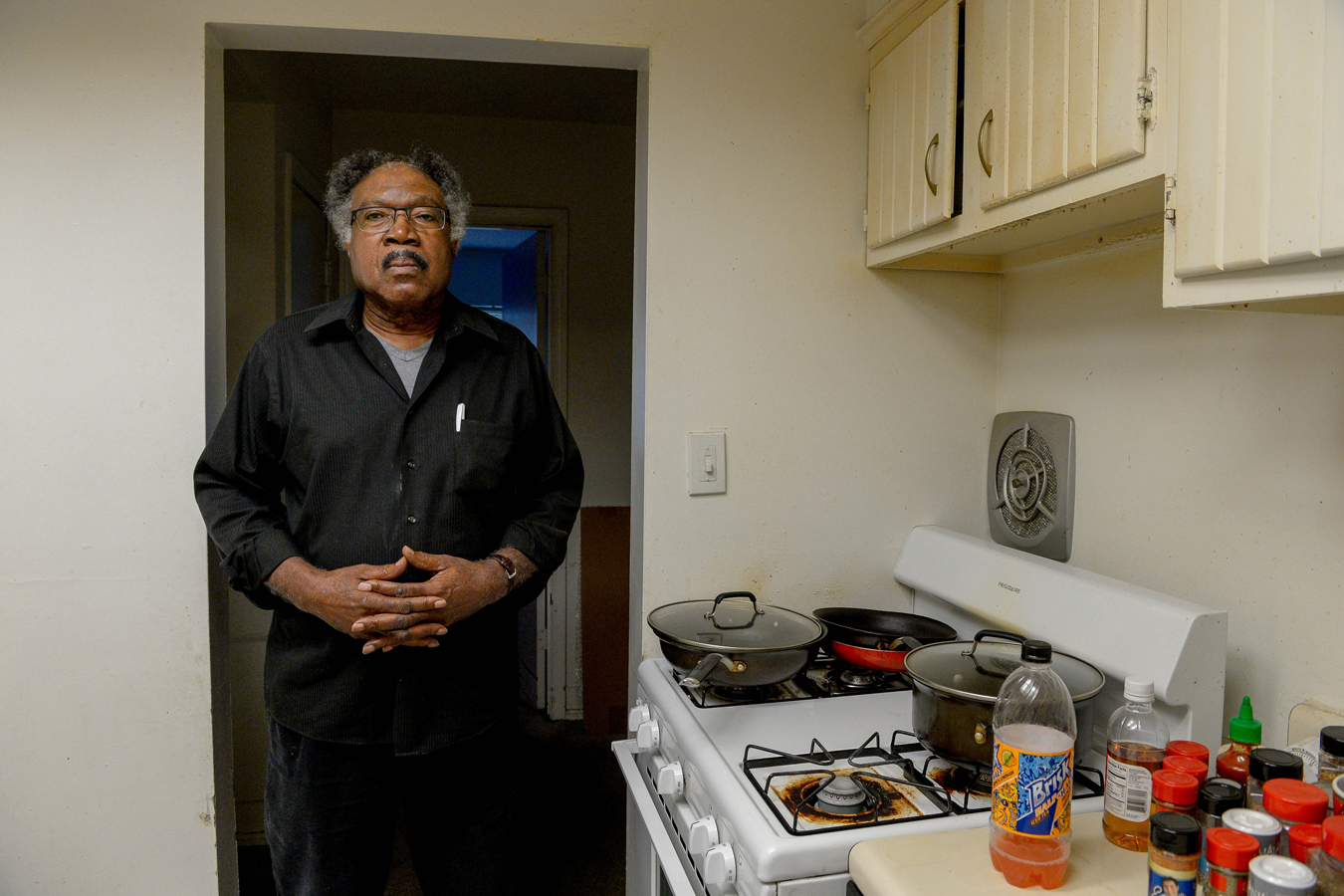
George Nelson lost his wife, Jeanette Nelson, in 2015 after complications from surgery at the Innovations Surgery Center in Rockville, Md. (Camille Fine/USA Today)
Owners In Charge
Hospitals have committees and administrators focused on making sure doctors’ skills are sharp and their insurance is in place. Surgery centers have similar rules, but the oversight is lacking when a controversial doctor is also the facility owner.
Dr. Paul Mackoul, a Maryland gynecological surgeon, lost his hospital privileges in 2001 after a medical staff committee at Washington Hospital Center reviewed his “competence or conduct,” according to Washington, D.C., Board of Medicine records. Mackoul criticized the decision, saying he never had a chance to defend himself.
Mackoul has faced 14 lawsuits since 1991 alleging substandard obstetrics and gynecological care, according to court records. Women have accused him of leaving them infertile, incontinent or with perforated bowels. Mackoul said in an email that settlements were paid on his behalf in four cases, two were decided in his favor at trial, one case is pending and the others were dismissed or resulted in no payment on his behalf.
Despite losing privileges at Washington Hospital Center, Mackoul and his wife, who is also a gynecologist, co-own and operate Innovations Surgery Center in Rockville, Md. The facility is Medicare-approved, based on the recommendation of an accreditation body.
An insurer’s lawsuit shows that in early 2015, Mackoul’s malpractice policy did not cover him to perform cancer surgery. Most hospital executives would not allow a physician to perform procedures that aren’t covered, according to interviews with hospital administration experts.
Mackoul, his wife and the facility administrator served as the governing board at Innovations, according to court records and Mackoul. He also said he has privileges at one Maryland hospital.
In February 2015, Jeanette Nelson, 73, a soprano gospel singer, turned to Mackoul for care after she had been diagnosed with uterine cancer.
He performed her hysterectomy without incident. Mackoul saw her again a month later to install a catheter in her chest that would better deliver chemotherapy drugs to her bloodstream. Nelson died in a hospital later that same day, her autopsy report says.
The autopsy report states that blood built up in Nelson’s chest wall and caused her lung to collapse, but the source of the blood was “not definitively identified.” However, the report concluded that her death was the result of “a complication of attempted treatment for her” cancer.
Nelson’s family alleged in a lawsuit that Mackoul punctured a vein as he installed the catheter, and his mistake caused internal bleeding that proved fatal.

Jeanette and George Nelson were married in 1966 on Belle Isle in Detroit. (Courtesy of George Nelson)

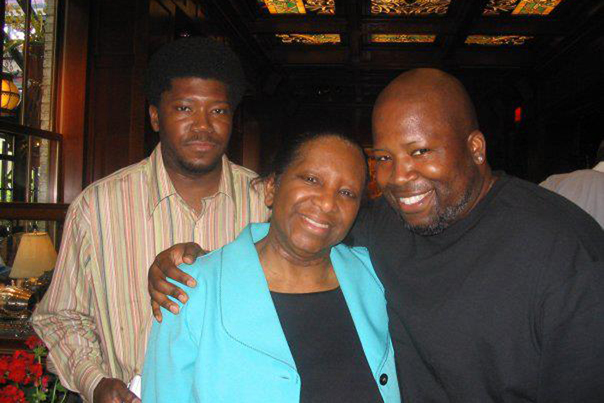
Jeanette Nelson celebrates Mother’s Day in 2007 with sons George Everett Nelson (left), now 49, and Dwayne Elliot Nelson, now 47. (Courtesy of George Everett Nelson)
George Nelson said he was devastated by the loss of his wife of 48 years, who was both devoutly religious and fascinated with murder-mystery detective shows. Before her death, the couple was looking forward to her graduation from a master’s program in cybersecurity policy.
After his wife’s passing, he said: “I didn’t care if I would have died.”
In an email, Mackoul said Jeanette Nelson’s death was related to a “major cardiac episode” and that experts he retained found no shortcomings with his care. He denied wrongdoing in the lawsuit, which reached a confidential settlement.
“Unfortunately, even under the best of circumstances and in the very best of hands, a patient can experience the most catastrophic event,” Mackoul said in an email.
Mackoul’s malpractice insurer sued him over the wrongful death case, revealing in court records that he had not been covered to perform cancer surgeries. Mackoul said in an email that the port procedure is not specifically a cancer surgery, though he was not aware of the clause at the time and was self-insured. He denied negligence in court filings, and the case reached a confidential settlement.
The question remains whether the center’s governing board was independent enough to perform the typical doctor-oversight practices, said Dr. Jonathan Burroughs, a faculty member of the American College of Healthcare Executives. And it’s a question that applies to an untold number of surgery centers.
“When push comes to shove,” he said, “the board has to make decisions in the best interest of the community and good patient care.”
KHN senior correspondent Jay Hancock contributed to this report.
This story was produced by Kaiser Health News, an editorially independent program of the Kaiser Family Foundation.