More than 625,000 people have enrolled in Covered California, state officials announced on Tuesday. “Milestone enrollment numbers,” blared a press release for the insurance exchange.
No other state comes close.
So it’s all the more puzzling that nearly no one fussed over another huge figure: the 680,000-plus residents who signed up for the state’s Low Income Health Plan — perhaps the biggest element of Obamacare that got the smallest share of attention.
“It’s frankly been the most underreported story in health reform,” Anthony Wright, executive director of Health Access, tells California Healthline.
Edge of the LIHP
Wright’s argument boils down to this: The LIHP provided immediate relief to some of California’s neediest residents, while teeing up broader health reform efforts.
“It jump-started the Medicaid expansion nationally with bigger numbers than projected,” Wright says, and it “helped us figure out a better way to do the safety net … a model for going forward with the remaining uninsured.”
And for those in the know, the LIHP’s existence also offered context during the exchange’s fraught rollout in October and November.
Even as observers were fretting about a shortfall of tens of thousands of sign-ups through Covered California, hundreds of thousands of Californians already were taking advantage of Obamacare’s coverage expansion, thanks to the LIHP.
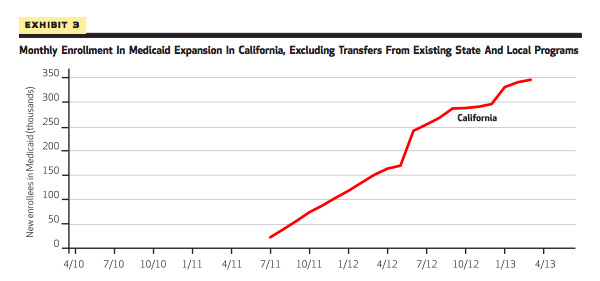
The program was conceived as part of the state’s “Bridge to Reform,” an initiative made possible with a Section 1115 waiver from CMS in November 2010, and began enrolling eligible California residents in July 2011. (Enrollees essentially had to make too much money to qualify for “traditional” Medicaid, but no more than about 138% of the federal poverty level.) Each county was offered an opportunity to create its own LIHP and some initially demurred, citing concerns about the ACA’s legality or their own liability.
Ultimately, about 20 different LIHPs were created; the state transitioned about 630,000 enrollees into Medi-Cal on Jan. 1, when the program expired. (An additional 24,000 enrollees were steered toward Covered California.)
The LIHP wasn’t alone in structure or ambition. Six other states made similar moves to expand their Medicaid programs ahead of the formal launch date, although their programs ended up being a fraction of the scope.
Yet despite its size and success, California’s LIHP was mostly ignored. Why? Blame the fickle nature of politics.
For most of the LIHP’s three-year lifespan, wonks and politicos focused their attention elsewhere — on Obamacare’s legal challenges or which states were saying yes to the Medicaid expansion. When the LIHP did grab headlines in late 2013, they mostly recounted how its glitches were another sign of the troubled Obamacare rollout that had captivated national conversation.
That was a big departure for the program, given that its routine hiccups in 2012 and 2013 weren’t fed through the funhouse mirror of national politics and went largely overlooked in California, too. For example, take ViaCare — Monterey County’s LIHP — which was originally slated to launch in early 2012 and cover 1,500 people; officials postponed it to spring 2013 and reduced their target to 300 enrollees. The delay barely made a ripple.
What We Can Learn From the LIHP
Overall, the LIHP laid a trail for Medicaid expansion, Wright and other advocates say. Health care providers now have more experience serving low-income patients, and some of the pent-up demand for health care services may have been alleviated.
“This program was critical to our preparation for the full ACA Medicaid expansion on January 1,” according to a recent statement from Toby Douglas, director of the state’s Department of Health Care Services. “It allowed us to strengthen our provider networks and expand our use of the more coordinated services provided by organized delivery systems.”
“This gave the state a head start,” adds Carol Sloan, a spokesperson for DHCS.
The 30 months of LIHP data also offer clues for what we can expect from the Medicaid expansion, not just in California but across the nation, too.
Lesson #1: Brace for steady, if sometimes slow enrollment
“The first big lesson is that enrollment in expansions like [the LIHP] takes a while,” Benjamin Sommers tells California Healthline.
Sommers, a Harvard professor, was the lead author of a new Health Affairs study that examined early Medicaid expansion in several states.
In California, “enrollment was still steadily increasing [two-to-three] years into the expansion,” Sommers notes. “So we shouldn’t be too quick to judge the success of failure of the Medicaid expansion until we have a longer time period to evaluate.”

This Program Was Bigger Than Covered California. Why Did We Ignore It?
Lesson #2: The sickest and oldest patients aggressively seek out coverage
Many of the initial enrollees in the LIHP were those with the most motivation to get covered, experts note.
About one-third of people who gained coverage through the program had chronic conditions, for example. And the age breakdown of LIHP enrollees was also notable; more than half were ages 45 and up.
Taken together, it’s a reminder that it’s not just the oldest and sickest who are more likely to seek out private coverage, like the new plans being sold through insurance exchanges, but all forms of new coverage available through the Affordable Care Act.
Lesson #3: Emergency department utilization will stabilize
The LIHP also has a chance to make a major contribution to the Obamacare canon: by offering data on whether coverage expansion reduces unnecessary utilization or merely adds demand to the health system.
There just hasn’t been much evidence either way, which is why so much attention has focused on data coming out of the Oregon Health Insurance Experiment. For example, researchers have puzzled over the eye-catching conclusion that Medicaid expansion in Oregon led to a surge in emergency visits.
However, that’s not quite what California’s LIHP found.
A recent report suggested that ED utilization was flat– or even fell — among LIHP enrollees, although more comprehensive data suggests that there was a short-lived spike. But that should be within expectations, suggested Gerald Kominski, director of UCLA’s Center for Health Policy Research.
“That behavior of seeking primary care in the ER has been reinforced for a period of years, and it doesn’t change immediately just because you give somebody an insurance card,” Kominski told the U-T San Diego‘s Paul Sisson recently.
Dylan Roby, Kominski’s colleague at UCLA, says that the center is preparing an “apples-to-apples” comparison of utilization between residents who had access to the safety net and those who didn’t, drawing on LIHP data.
“In those analyses, which are preliminary, we do see an initial increase in [ED], outpatient, and [inpatient] use that stabilizes over time,” Roby tells California Healthline.
Looking Ahead
The LIHP’s legacy can be seen in Medi-Cal’s rapid growth. In addition to the LIHP’s infusion of enrollees, another 584,000 Californians residents were deemed eligible for the state’s Medicaid program through the Covered California exchange. And experts say that providers and managed care plans’ experience working with LIHP enrollees will prove valuable for redesigning care management and delivery to this underserved population.
But the legacy of the “most under-reported story” in health reform also could offer takeaways for how the next big coverage expansion gets covered in the press.
“We should be less concerned on a month-by-month basis whether or not the law meets predetermined, [imprecise] benchmarks” Harvard’s Sommers says, “and instead keep an eye on the big picture of what coverage expansion is doing for those gaining insurance.”
Weekly Roundup
Here’s what else is making news on the road to reform.
Looking at a loophole: At the Incidental Economist, Adrianna McIntyre explores how the Affordable Care Act’s loophole for “mini-med” plans works. (With an able assist from Tim Jost.)
Employers cutting back on coverage: Bloomberg‘s Alex Wayne reports that Target will drop health coverage for its part-time workers ahead of new ACA regulations, following the lead of several other major companies.
Why the ACA is a boon for health plans: The Washington Post‘s Sarah Kliff explains that health insurers are only seeing Obamacare as a positive.
How the law’s helping: At the New York Times, Sabrina Tavernise reviews how expanding Medicaid coverage has brought relief to rural West Virginians.