

LOS ANGELES — They distribute GPS devices so they can track their homeless patients. They stock their street kits with glass pipes used to smoke meth, crack, or fentanyl. They keep company credit cards on hand in case a patient needs emergency food or water, or an Uber ride to the doctor.
These doctors, nurses, and social workers are fanning out on the streets of Los Angeles to provide health care and social services to homeless people — foot soldiers of a new business model taking root in communities around California.
Their strategy: Build trust with homeless people to deliver medicine wherever they are — and make money doing it.
“The biggest population of homeless people in this country is here in Southern California,” said Sachin Jain, a former Obama administration health official who is CEO of SCAN Group, which runs a Medicare Advantage insurance plan covering about 300,000 people in California, Arizona, Nevada, Texas, and New Mexico.
“The fastest-growing segment of people experiencing homelessness is actually older adults,” he said. “I said, ‘We’ve got to do something about this.’”
Jain’s organization three years ago created Healthcare in Action, a medical group that sends practitioners onto California’s streets solely to care for homeless people. It has grown rapidly, building operations in 17 communities, including Long Beach, West Hollywood, and San Bernardino County.
Since its launch, Healthcare in Action has cared for about 6,700 homeless patients and managed roughly 77,000 diagnoses, from schizophrenia to diabetes. It has placed about 300 people into permanent or temporary housing.

Street medicine in most of the country is practiced as a charitable endeavor, aimed at serving a challenging patient population failed by traditional medicine, its proponents say. Living transient, chaotic lives, homeless people suffer disproportionately from mental illness, addiction, and chronic disease and often don’t have health insurance — or don’t use it if they do.
That makes designing a business around caring for them a risk, insurance executives and health economists say.
“It’s really innovative and entrepreneurial to take all this energy and grit to try and improve things for a population that is too often ignored,” said Mark Duggan, a professor of economics at Stanford University who specializes in homelessness and Medicaid policy. “Financial incentives matter massively in health care. It’s everything.”
An estimated 181,000 people were homeless in California in 2023 — about 30% of the nation’s total. The number living outside, more than two-thirds of California’s total, increased 6.9% over the previous year.
The state’s leaders, including Democratic Gov. Gavin Newsom, have struggled to make inroads against the mounting public health and political crisis — despite marshaling unprecedented taxpayer resources.
“We have a huge problem on our hands, and we have a lot of health plans and municipalities saying, ‘We need you,’” Jain said.
On the Streets
On a cloudy April morning in Long Beach, Daniel Speller navigated his mobile medical van among the tents and tarps that crowded residential streets, searching for a couple of homeless patients. A physician assistant for Healthcare in Action, Speller said he was particularly worried about the badly infected wounds they developed on their limbs after they used the street drug xylazine, an animal tranquilizer often mixed with fentanyl.
“These wounds are everywhere. It’s really bad,” Speller said. If infections progress, they can require toe, foot, or arm amputations.
“Man, this one is still so deep,” Speller said as he peeled denim pants from the swollen leg of Robert Smith, 66.
After cleaning and wrapping Smith’s leg, Speller asked him if he needed anything else. “I lost my food stamps,” Smith replied.
Within the hour, Speller’s team of social workers and nurses had summoned an Uber to take Smith to a state office, where he received a new CalFresh card.




Speller then turned his medical van onto a side street lined with more tents and cars-turned-shelters. Nick Destry Anderson, 46, was sleeping on the sidewalk and badly in need of wound care.
“I was so scared. I thought I was going to lose my leg before I met them,” Anderson said, grimacing as Speller sprayed his leg with antibiotic mist. “These people saved my life.”
Anderson reported feeling lightheaded, so Speller asked another team member to use the company credit card to get him a cheeseburger and a Sprite.
Many homeless people languish on the streets, so entrenched in mental health crises or addiction that they don’t much care about seeing a doctor or taking their medication. Chronic diseases worsen. Wounds grow infected. People overdose or die from treatable conditions.
Part of street medicine is bandaging infected sores, administering antipsychotic injections, and treating chronic diseases. Street providers often hand out drug paraphernalia such as clean needles and glass pipes to reduce sharing and prevent infections. Perhaps more importantly, these workers build trust.
Getting homeless patients established with primary care doctors and nurses — who visit them on the streets, in parks, or wherever they happen to be — can prevent frequent and expensive emergency room trips and hospitalizations, potentially saving money for insurers and taxpayers, Jain argues. Even though shelter and housing are scarce, Healthcare in Action’s goal is to get patients healthy enough to live stable, independent lives, he said.
But that’s easier said than done. In West Hollywood that week in April, Healthcare in Action clinical coordinator Isabelle Peng found Lisa Vernon, a homeless woman, slumped over in her wheelchair at a busy bus stop. Vernon is a regular at nearby Cedars-Sinai Medical Center, Peng and her colleague David Wong said.
When Peng and Wong attempted to examine her swollen leg, Vernon shouted at them and declined aid. “Antibiotics aren’t going to save my life!” Vernon yelled as a mouse scurried for the potato chip shrapnel at her feet.
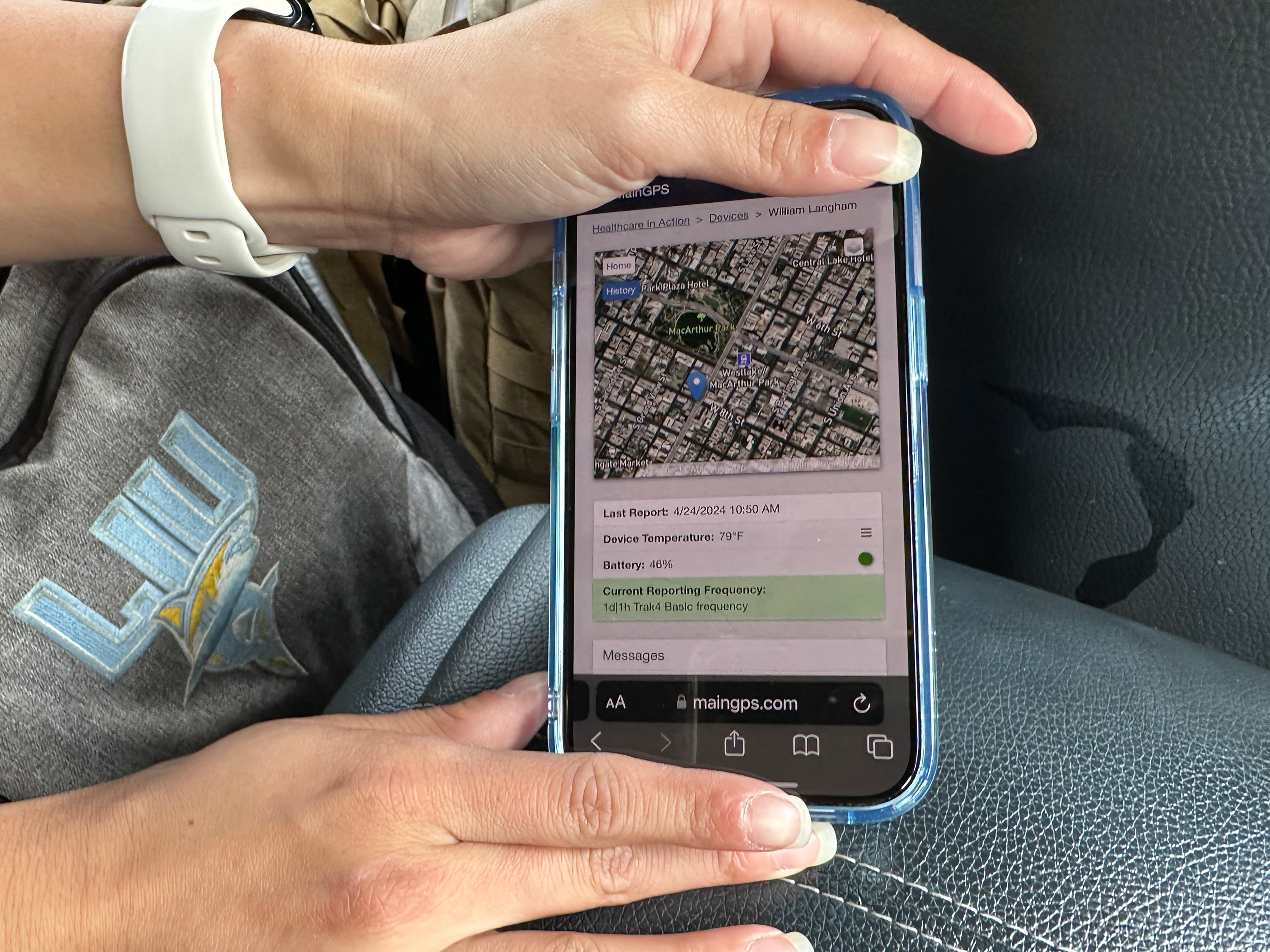
They moved on to their next patient, a man they were tracking with a GPS device they sometimes affix to homeless people’s belongings. Use of the devices is voluntary. They work better than cellphones because they less often get taken by law enforcement during encampment sweeps or stolen by thieves.
“Our patients really move around a lot, so this helps us go find them when we have to get them medication or do follow-up care,” Wong said. “We have already developed rapport with these patients, and they want us to see them.”


Growing Revenue
Street medicine teams are in demand, largely because of growing public frustration with homelessness. The city of West Hollywood, for instance, awarded Healthcare in Action a three-year contract that pays $47,000 a month. The nonprofit can also bill Medi-Cal, California’s Medicaid program, which covers low-income people, for its services.
Mari Cantwell, a health care consultant who served as California’s Medicaid director from 2015 until early 2020, said Medicaid reimbursements alone aren’t enough to fund street medicine providers. To remain viable, she said, they need to take creative financial steps, like Healthcare in Action has.
“Medicaid is never going to pay high margins, so you have to think about how to sustain things,” she said.
Healthcare in Action brought in about $2 million in revenue in its first year, $6 million in 2022, and $15.4 million in 2023, according to Michael Plumb, SCAN Group’s chief financial officer.
Healthcare in Action and SCAN’s Medicare Advantage insurance plan generate revenue by serving homeless patients in multiple ways:
- Both are tapping into billions of dollars in Medicaid money that states and the federal government are spending to treat homeless people in the field and to provide new social services like housing and food assistance.
For instance, Healthcare in Action has received $3.8 million from Newsom’s $12 billion Medicaid initiative called CalAIM, which allows it to hire social workers, doctors, and providers for street medicine teams, according to the state.
It also contracts with health insurers, including L.A. Care and Molina Healthcare in Southern California, to identify housing for homeless patients, negotiate with landlords, and provide financial help such as covering security deposits. - Healthcare in Action collects charitable donations from some hospitals and insurers, including CalOptima in Orange County and its own Medicare Advantage plan, SCAN Health Plan.
- Healthcare in Action partners with cities and hospitals to provide treatment and services. In 2022, it kicked off a contract with Cedars-Sinai to care for patients milling outside the hospital.
- It also enrolls eligible homeless patients into SCAN Health Plan because many low-income, older people qualify for both Medicaid and Medicare coverage. The plan had revenue of $4.9 billion in 2023, up from $3.5 billion in 2021.
“There’s been an incredible market fit, unfortunately,” Jain said. “You can’t walk or drive down a street in Los Angeles, rich or poor, and not run into this problem.”
Jim Withers, who coined the term “street medicine” decades ago and cares for homeless people in Pittsburgh, welcomed the entry of more providers given the enormous need. But he cautioned against a model with financial motives.
“I do worry about the corporatization of street medicine and capitalism invading what we’ve been building, largely as a social justice mission outside of the traditional health care system,” he said. “But nobody owns the streets, and we have to figure out how to play nice together.”