
When Larry Anders moved into the Bay at Burlington nursing home in late 2017, he wasn’t supposed to be there long. At 77, the stoic Wisconsin machinist had just endured the death of his wife of 51 years and a grim new diagnosis: throat cancer, stage 4.
His son and daughter expected him to stay two weeks, tops, before going home to begin chemotherapy. From the start, they were alarmed by the lack of care at the center, where, they said, staff seemed indifferent, if not incompetent — failing to check on him promptly, handing pills to a man who couldn’t swallow.
Anders never mentioned suicide to his children, who camped out day and night by his bedside to monitor his care.
But two days after Christmas, alone in his nursing home room, Anders killed himself. He didn’t leave a note.
The act stunned his family. His daughter, Lorie Juno, 50, was so distressed that, a year later, she still refused to learn the details of her father’s death. The official cause was asphyxiation.
“It’s sad he was feeling in such a desperate place in the end,” Juno said.
In a nation where suicide continues to climb, claiming more than 47,000 lives in 2017, such deaths among older adults — including the 2.2 million who live in long-term care settings — are often overlooked. A six-month investigation by Kaiser Health News and PBS NewsHour finds that older Americans are quietly killing themselves in nursing homes, assisted living centers and adult care homes.
If You Need Help
If you or someone you know has talked about contemplating suicide, call the National Suicide Prevention Lifeline at 1-800-273-8255, or use the online Lifeline Crisis Chat, both available 24 hours a day, seven days a week.
People 60 and older can call the Institute on Aging’s 24-hour, toll-free Friendship Line at 800-971-0016. IOA also makes ongoing outreach calls to lonely older adults.
Poor documentation makes it difficult to tell exactly how often such deaths occur. But a KHN analysis of new data from the University of Michigan suggests that hundreds of suicides by older adults each year — nearly one per day — are related to long-term care. Thousands more people may be at risk in those settings, where up to a third of residents report suicidal thoughts, research shows.
Each suicide results from a unique blend of factors, of course. But the fact that frail older Americans are managing to kill themselves in what are supposed to be safe, supervised havens raises questions about whether these facilities pay enough attention to risk factors like mental health, physical decline and disconnectedness — and events such as losing a spouse or leaving one’s home. More controversial is whether older adults in those settings should be able to take their lives through what some fiercely defend as “rational suicide.”
Tracking suicides in long-term care is difficult. No federal regulations require reporting of such deaths and most states either don’t count — or won’t divulge — how many people end their own lives in those settings.
Briana Mezuk, an associate professor of epidemiology at the University of Michigan, found in 2015 that the rate of suicide in older adults in nursing homes in Virginia was nearly the same as the rate in the general population, despite the greater supervision the facilities provide.
In research they presented at the 2018 Gerontological Society of America annual meeting, Mezuk’s team looked at nearly 50,000 suicides among people 55 and older in the National Violent Death Reporting System (NVDRS) from 2003 to 2015 in 27 states. They found that 2.2% of those suicides were related to long-term care. The people who died were either people living in or transitioning to long-term care, or caregivers of people in those circumstances.

Briana Mezuk (Courtesy of University of Michigan School of Public Health)
KHN extrapolated the finding to the entire U.S., where 16,500 suicides were reported among people 55 and older in 2017, according to federal figures. That suggests that at least 364 suicides a year occur among people living in or moving to long-term care settings, or among their caregivers. The numbers are likely higher, Mezuk said, since the NVDRS data did not include such states as California and Florida, which have large populations of elders living in long-term care sites.
But representatives of the long-term care industry point out that by any measure, such suicides are rare.
The deaths are “horrifically tragic” when they occur, said Dr. David Gifford, of the American Health Care Association. But, he added, the facilities offer “a very supervised environment,” and settings that receive Medicare or Medicaid funding are required to assess and monitor patients for suicidal behavior.
“I think the industry is pretty attuned to it and paying attention to it,” Gifford said, noting that mental health issues among older adults in general must be addressed. “I don’t see this data as pointing to a problem in the facilities.”
KHN examined over 500 attempted and completed suicides in long-term care settings from 2012 to 2017 by analyzing thousands of death records, medical examiner reports, state inspections, court cases and incident reports.
Even in supervised settings, records show, older people find ways to end their own lives. Many used guns, sometimes in places where firearms weren’t allowed or should have been securely stored. Others hanged themselves, jumped from windows, overdosed on pills or suffocated themselves with plastic bags. (The analysis did not examine medical aid-in-dying, a rare and restricted method by which people who are terminally ill and mentally competent can get a doctor’s prescription for lethal drugs. That is legal only in seven states and the District of Columbia.)
Descriptions KHN unearthed in public records shed light on residents’ despair: Some told nursing home staff they were depressed or lonely; some felt that their families had abandoned them or that they had nothing to live for. Others said they had just lived long enough: “I am too old to still be living,” one patient told staff. In some cases, state inspectors found nursing homes to blame for failing to heed suicidal warning signs or evicting patients who tried to kill themselves.
A better understanding is crucial: Experts agree that late-life suicide is an under-recognized problem that is poised to grow.
By 2030, all baby boomers will be older than 65 and 1 in 5 U.S. residents will be of retirement age, according to census data. Of those who reach 65, two-thirds can expect to need some type of long-term care. And, for poorly understood reasons, that generation has had higher rates of suicide at every stage, said Dr. Yeates Conwell, director of the Office for Aging Research and Health Services at the University of Rochester.
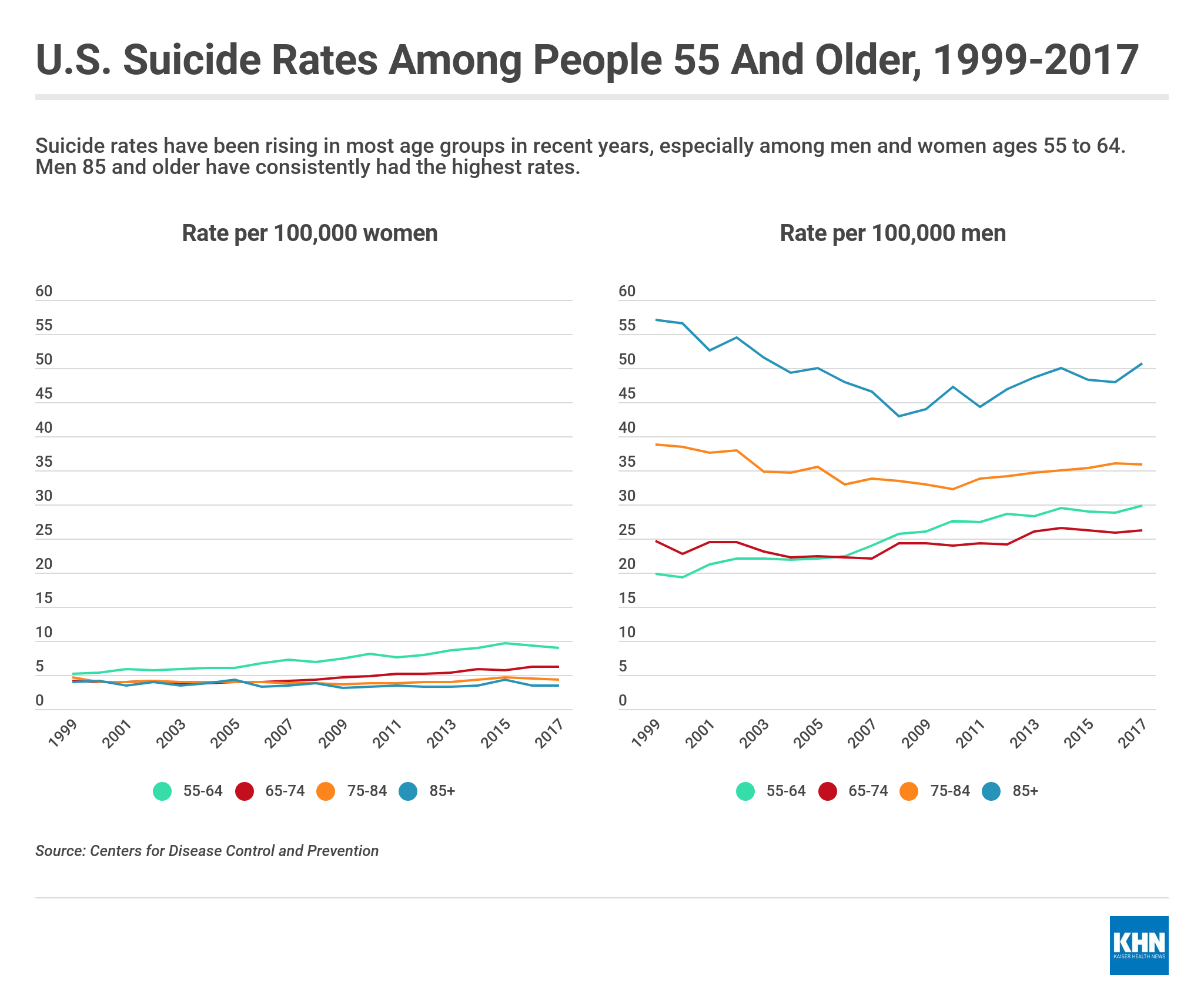
“The rise in rates in people in middle age is going to be carried with them into older adulthood,” he said.
Long-term care settings could be a critical place to intervene to avert suicide — and to help people find meaning, purpose and quality of life, Mezuk argued: “There’s so much more that can be done. It would be hard for us to be doing less.”
In Wisconsin, Larry Anders’ children chose to speak publicly because they felt the nursing home failed their father.
Anders, a taciturn Army veteran, lived a low-key retirement in Waukesha, outside of Milwaukee. He grew asparagus, watched “Wheel of Fortune” with his wife, Lorna, in matching blue recliners and played the slot machines at a Chinese restaurant.
Following the November 2017 death of his wife, and his throat cancer diagnosis, he initially refused treatment, but then agreed to give it a try.
Anders landed at the Bay at Burlington, 40 minutes from his home, the closest facility his Medicare Advantage plan would cover. The first day, Lorie Juno grew worried when no one came to greet her father after the ambulance crew wheeled him to his room. The room had no hand sanitizer and the sink had no hot water.
In his week in the Burlington, Wis., center, Anders wrestled with anxiety and insomnia. Anders, who rarely complained, called his daughter in a panic around 2 a.m. one day, saying that he couldn’t sleep and that “they don’t know what the hell they’re doing here,” according to Juno. When she called, staff assured her that Anders had just had a “snack,” which she knew wasn’t true because he ate only through a feeding tube.
His children scrambled to transfer him elsewhere, but they ran out of time. On Dec. 27, Mike Anders, 48, woke up in an armchair next to his father’s bed after spending the night. He left for his job as a machinist between 5 and 6 a.m. At 6:40 a.m., Larry Anders was found dead in his room.
“I firmly believe that had he had better care, it would’ve been a different ending,” Mike Anders said.
Research shows events like losing a spouse and a new cancer diagnosis put people at higher risk of suicide, but close monitoring requires resources that many facilities don’t have.

“It’s sad he was feeling in such a desperate place in the end,” says Lorie Juno of her father, Larry Anders.(Darren Hauck for KHN)

Larry Anders, a machinist and an Army veteran, enjoyed growing asparagus and playing slot machines.(Darren Hauck for KHN)

“I firmly believe that had he had better care, it would’ve been a different ending,” says Mike Anders of his father, Larry Anders.(Darren Hauck for KHN)
Nursing homes already struggle to provide enough staffing for basic care. Assisted living centers that promote independence and autonomy can miss warning signs of suicide risk, experts warn.
In the weeks before and after Anders’ death, state inspectors found a litany of problems at the facility, including staffing shortages. When inspectors found a patient lying on the floor, they couldn’t locate any staff in the unit to help.
Champion Care, the New York firm that runs the Bay at Burlington and other Wisconsin nursing homes, noted that neither police nor state health officials found staff at fault in Anders’ death.
Merely having a suicide on-site does not mean a nursing home broke federal rules. But in some suicides KHN reviewed, nursing homes were penalized for failing to meet requirements for federally funded facilities, such as maintaining residents’ well-being, preventing avoidable accidents and telling a patient’s doctor and family if they are at risk of harm.
For example:
- An 81-year-old architect fatally shot himself while his roommate was nearby in their shared room in a Massachusetts nursing home in 2016. The facility was fined $66,705.
- A 95-year-old World War II pilot hanged himself in an Ohio nursing home in 2016, six months after a previous attempt in the same location. The facility was fined $42,575.
- An 82-year-old former aircraft mechanic, who had a history of suicidal ideation, suffocated himself with a plastic bag in a Connecticut nursing home in 2015. The facility was fined $1,020.
Prevention needs to start long before these deaths occur, with thorough screenings upon entry to the facilities and ongoing monitoring, Conwell said. The main risk factors for senior suicide are what he calls “the four D’s”: depression, debility, access to deadly means and disconnectedness.
“Pretty much all of the factors that we associate with completed suicide risk are going to be concentrated in long-term care,” Conwell said.
Most seniors who choose to end their lives don’t talk about it in advance, and they often die on the first attempt, he said.
That was the case for the Rev. Milton P. Andrews Jr., a former Seattle pastor, who “gave no hint” he wanted to end his life six years ago at a Wesley Homes retirement center in nearby Des Moines, Wash. Neither his son, Paul Andrews, nor the staff at the center had any suspicions, they said.
“My father was an infinitely deliberate person,” said Paul Andrews, 69, a retired Seattle journalist. “There’s no way once he decided his own fate that he was going to give a clue about it, since that would have defeated the whole plan.”
At 90, the Methodist minister and human rights activist had a long history of making what he saw as unpopular but morally necessary decisions. He drew controversy in the pulpit in the 1950s for inviting African Americans into his Seattle sanctuary. He opposed the Vietnam War and was arrested for protesting nuclear armament. His daughter was once called a “pinko” because Andrews demanded equal time on a local radio station to rebut a conservative broadcaster.
In 2013, facing a possible second bout of congestive heart failure and the decline of his beloved wife, Ruth, who had dementia, Andrews made his final decision. On Valentine’s Day, he took a handful of sleeping pills, pulled a plastic bag over his head and died.
Milton Andrews wrote a goodbye note on the cover of his laptop computer in bold, black marker.
“Fare-well! I am ready to die! I choose this ‘shortcut,’” it read in part. “I love you all, and do not wish a long, protracted death — with my loved ones waiting for me to die.”

Retired Seattle minister Milt Andrews, 90, ended his life on Valentine’s Day 2013 at his assisted living center, leaving behind a note written in black marker on the cover of his laptop computer.(Dan DeLong for KHN)
Christine Tremain, a spokeswoman for Wesley Homes, said Andrews’ death has been the only suicide reported in her 18 years at the center.
“Elder suicide is an issue that we take seriously and work to prevent through the formal and informal support systems that we have in place,” she said.
At first, Paul Andrews said he was shocked, devastated and even angry about his dad’s death. Now, he just misses him.
“I always feel like he was gone too soon, even though I don’t think he felt like that at all,” he said.
Andrews has come to believe that elderly people should be able to decide when they’re ready to die.
“I think it’s a human right,” he said. “If you go out when you’re still functioning and still have the ability to choose, that may be the best way to do it and not leave it to other people to decide.”

Paul Andrews was shocked when his father, the Rev. Milton P. Andrews Jr., died by suicide at a Seattle-area assisted living center in 2013. He has since come to believe that elderly people should be able to decide when they’re ready to die.(Dan DeLong for KHN)
That’s a view shared by Dena Davis, 72, a bioethics professor at Lehigh University in Pennsylvania. Suicide “could be a rational choice for anyone of any age if they feel that the benefits of their continued life are no longer worth it,” she said.
“The older you get, the more of your life you’ve already lived — hopefully, enjoyed — the less of it there is to look forward to,” said Davis, who has publicly discussed her desire to end her own life rather than die of dementia, as her mother did.
But Conwell, a leading geriatric psychiatrist, finds the idea of rational suicide by older Americans “really troublesome.” “We have this ageist society, and it’s awfully easy to hand over the message that they’re all doing us a favor,” he said.
When older adults struggle with mental illness, families often turn to long-term care to keep them safe.
A jovial social worker who loved to dance, Ellen Karpas fell into a catatonic depression after losing her job at age 74 and was diagnosed with bipolar disorder. Concerned that she was “dwindling away” at home, losing weight and skipping medications, her children persuaded her to move to an assisted living facility in Minneapolis in 2017.
Karpas enjoyed watching the sunset from the large, fourth-story window of her room at Ebenezer Loren on Park. But she had trouble adjusting to the sterile environment, according to son Timothy Schultz, 52.
“I do not want to live here for the rest of my life,” she told him.

Ellen Karpas (second from left) and four of her five children attend a St. Patrick’s Day parade in 2016. The following year, the 79-year-old died by suicide at an assisted living facility in Minneapolis. (Courtesy of Timothy Schultz)
On Oct. 4, 2017, less than a month after she moved in, Karpas was unusually irritable during a visit, her daughter, Sandy Pahlen, 54, recalled. Pahlen and her husband left the room briefly. When they returned, Karpas was gone. Pahlen looked out an open window and saw her mother on the ground below.
Karpas, 79, was declared dead at the scene.
Schultz said he thinks the death was premeditated, because his mother took off her eyeglasses and pulled a stool next to the window. Escaping was easy: She just had to retract a screen that rolled up like a roller blind and open the window with a hand crank.
Pahlen said she believes medication mismanagement — the staff’s failure to give Karpas her regular mood stabilizer pills — contributed to her suicide. But a state health department investigation found staffers were not at fault in the death. Eric Schubert, a spokesman for Fairview Health Services, which owns the facility, called Karpas’ death “very tragic” but said he could not comment further because the family has hired a lawyer. Their lawyer, Joel Smith, said the family plans to sue the facility and may pursue state legislation to make windows suicide-proof at similar places.
“Where do I even begin to heal from something that is so painful, because it was so preventable?” said Raven Baker, Karpas’ 26-year-old granddaughter.
Nationwide, about half of people who die by suicide had a known mental health condition, according to the Centers for Disease Control and Prevention. Mental health is a significant concern in U.S. nursing homes: Nearly half of residents are diagnosed with depression, according to a 2013 CDC report.
That often leads caregivers, families and patients themselves to believe that depression is inevitable, so they dismiss or ignore signs of suicide risk, said Conwell.
“Older adulthood is not a time when it’s normal to feel depressed. It’s not a time when it’s normal to feel as if your life has no meaning,” he said. “If those things are coming across, that should send up a red flag.”

Roland K. Tiedemann was 89 when he took his life on Jan. 22, 2018, at a Wenatchee, Wash., assisted living center. The action shocked his daughter, Jane Davis, and left a void in the life of her daughter, Jayna, shown here at age 7½ in December 2014. (Courtesy of Jane Davis)
Still, not everyone with depression is suicidal, and some who are suicidal don’t appear depressed, said Julie Rickard, a psychologist in Wenatchee, Wash., who founded a regional suicide prevention coalition in 2012. She’s launching one of the nation’s few pilot projects to train staff and engage fellow residents to address suicides in long-term care.
In the past 18 months, three suicides occurred at assisted living centers in the rural central Washington community of 50,000 people. That included Roland K. Tiedemann, 89, who jumped from the fourth-story window of a local center on Jan. 22, 2018.
“He was very methodical. He had it planned out,” Rickard said. “Had the staff been trained, they would have been able to prevent it. Because none of them had been trained, they missed all the signs.”
Tiedemann, known as “Dutch,” lived there with his wife, Mary, who has dementia. The couple had nearly exhausted resources to pay for their care and faced moving to a new center, said their daughter, Jane Davis, 45, of Steamboat Springs, Colo. Transitions into or out of long-term care can be a key time for suicide risk, data shows.
After Tiedemann’s death, Davis moved her mother to a different facility in a nearby city. Mary Tiedemann, whose dementia is worse, doesn’t understand that her husband died, Davis said. “At first I would tell her. And I was telling her over and over,” she said. “Now I just tell her he’s hiking.”
At the facility where Tiedemann died, Rickard met with the residents, including many who reported thoughts of suicide.

Julie Rickard (Frank Carlson/PBS NewsHour)
“The room was filled with people who wanted to die,” she said. “These people came to me to say: ‘Tell me why I should still live.’”
Most suicide prevention funding targets young or middle-aged people, in part because those groups have so many years ahead of them. But it’s also because of ageist attitudes that suggest such investments and interventions are not as necessary for older adults, said Jerry Reed, a nationally recognized suicide expert with the nonprofit Education Development Center.
“Life at 80 is just as possible as life at 18,” Reed said. “Our suicide prevention strategies need to evolve. If they don’t, we’re going to be losing people we don’t need to lose.”
Even when there are clear indications of risk, there’s no consensus on the most effective way to respond. The most common responses — checking patients every 15 minutes, close observation, referring patients to psychiatric hospitals — may not be effective and may even be harmful, research shows.
But intervening can make a difference, said Eleanor Feldman Barbera, a New York psychologist who works in long-term care settings.
She recalled a 98-year-old woman who entered a local nursing home last year after suffering several falls. The transition from the home she shared with her elderly brother was difficult. When the woman developed a urinary tract infection, her condition worsened. Anxious and depressed, she told an aide she wanted to hurt herself with a knife. She was referred for psychological services and improved. Weeks later, after a transfer to a new unit, she was found in her room with the cord of a call bell around her neck.
After a brief hospitalization, she returned to the nursing home and was surrounded by increased care: a referral to a psychiatrist, extra oversight by aides and social workers, regular calls from her brother. During weekly counseling sessions, the woman now reports she feels better. Barbera considers it a victory.
“She enjoys the music. She hangs out with peers. She watches what’s going on,” Barbera said. “She’s 99 now — and she’s looking toward 100.”
If you or someone you know has talked about contemplating suicide, call the National Suicide Prevention Lifeline at 1-800-273-8255, or use the online Lifeline Crisis Chat, both available 24 hours a day, seven days a week.
People 60 and older can call the Institute on Aging’s 24-hour, toll-free Friendship Line at 800-971-0016. IOA also makes ongoing outreach calls to lonely older adults.
This story was produced by Kaiser Health News, an editorially independent program of the Kaiser Family Foundation.